Clinical features of Kawasaki Disease
Would you like to find out what those-in-the-know have to say about Kawasaki,Disease,children,clinical.lymph.node,syndrome? The information in the article below comes straight from well-informed experts with special knowledge about Kawasaki,Disease,children,clinical.lymph.node,syndrome.
So far, we've uncovered some interesting facts about Kawasaki,Disease,children,clinical.lymph.node,syndrome. You may decide that the following information is even more interesting.
Kawasaki disease (KD), formerly known as mucocutaneous lymph node syndrome and infantile polyarteritis nodosa, is an acute febrile vasculitis of childhood.
Kawasaki disease is the leading cause of acquired heart disease in children in the United States and Japan.
Fever is characteristically high (104°F or higher), remittent, and unresponsive to antibiotics. The duration of fever without treatment is generally 1–2 wk, but it may persist for 3–4 wk. Prolonged fever is prognostic for the development of coronary artery disease.
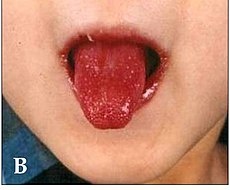
In addition to fever, the five characteristic features of Kawasaki disease are: bilateral bulbar conjunctival injection, usually without exudate; erythema of the oral and pharyngeal mucosa with strawberry tongue and dry, cracked lips, and without ulceration; edema and erythema of the hands and feet; rash of various forms (maculopapular, erythema multiforme, or scarlatiniform) with accentuation in the groin area; and nonsuppurative cervical lymphadenopathy, usually unilateral, with node size of ?1.5 cm.
Perineal desquamation is common in the acute phase. Periungual desquamation of the fingers and toes begins 1–3 wk after the onset of illness and may progress to involve the entire hand and foot.
Other features include extreme irritability that is especially prominent in infants, aseptic meningitis, diarrhea, mild hepatitis, hydrops of the gallbladder, urethritis and meatitis with sterile pyuria, otitis media, and arthritis. Arthritis may occur early in the illness or may develop in the 2nd–3rd week, generally affecting hands, knees, ankles, or hips. It is self-limited but may persist for several weeks.
Cardiac involvement is the most important manifestation of Kawasaki disease. Myocarditis, manifested as tachycardia out of proportion to fever occurs in at least 50% of patients; decreased ventricular function occurs in a smaller number of patients. Pericarditis with a small pericardial effusion is common during the acute illness. Coronary artery aneurysms develop in up to 25% of untreated patients in the 2nd–3rd wk of illness and are best detected by two-dimensional echocardiography. Giant coronary artery aneurysms (?8 mm internal diameter) pose the greatest risk for rupture, thrombosis or stenosis, and myocardial infarction . Significant valvular regurgitation and systemic artery aneurysms may occur but are uncommon. Axillary, popliteal, or other arteries may also be involved and manifest as a localized pulsating mass.
Clinical Phases of Disease:
Kawasaki disease is generally divided into three clinical phases.
The acute febrile phase, which usually lasts 1–2 wk, is characterized by fever and the other acute signs of illness. The dominant cardiac manifestation is myocarditis. In addition, a macrophage activation syndrome may rarely be evident .
The subacute phase begins when fever and other acute signs have abated, but irritability, anorexia, and conjunctival injection may persist. The subacute phase is associated with desquamation, thrombocytosis, the development of coronary aneurysms, and the highest risk of sudden death in those who have developed aneurysms. This phase generally lasts until about the 4th wk.
The convalescent phase begins when all clinical signs of illness have disappeared and continues until the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) return to normal, ?6–8 wk after the onset of illness.
Certain clinical and laboratory findings may predict a more severe outcome. These include male gender, age <1 yr, prolonged fever, recrudescence of fever after an afebrile period, and the following laboratory values at presentation: low hemoglobin or platelet levels, high neutrophil and band counts, hyponatremia, and low albumin and age-adjusted serum IgG levels. Scoring systems based on these factors, however, have not proven sufficiently sensitive for selective treatment of patients based on risk.
Don't limit yourself by refusing to learn the details about Kawasaki,Disease,children,clinical.lymph.node,syndrome. The more you know, the easier it will be to focus on what's important.
 Subscribe to email feed
Subscribe to email feed












